I was just catching up on emails and saw this item from Nature.
I do not have the permission to share the whole article with you but feel that it is alright to share these two paragraphs:
Keith Krehbiel lived with Parkinson’s disease for nearly 25 years before agreeing to try a brain implant that might alleviate his symptoms. He had long been reluctant to submit to the surgery. “It was a big move,” he says. But by 2020, his symptoms had become so severe that he grudgingly agreed to go ahead.
Deep-brain stimulation involves inserting thin wires through two small holes in the skull into a region of the brain associated with movement. The hope is that by delivering electrical pulses to the region, the implant can normalize aberrant brain activity and reduce symptoms. Since the devices were first approved almost three decades ago, some 200,000 people have had them fitted to help calm the tremors and rigidity caused by Parkinson’s disease. But about 40,000 of those who received devices made after 2020 got them with a special feature that has largely not yet been turned on. The devices can read brain waves and then adapt and tailor the rhythm of their output, in much the same way as a pacemaker monitors and corrects the heart’s electrical rhythms, says Helen Bronte-Stewart, a neurologist at Stanford University in California.
I am going to try and contact Helen at Stanford University to gather more details and, hopefully, to obtain her permission to share the complete article with you.
As you know, Jean suffers from PD and was diagnosed in 2015.
Very recently there was this article on PD and I reproduce parts of it (I have not applied for permission to republish) but I have provided the link to a pdf.
ooOOoo
Protein discovery linked to Parkinson’s disease opens future research areas
by WEHI
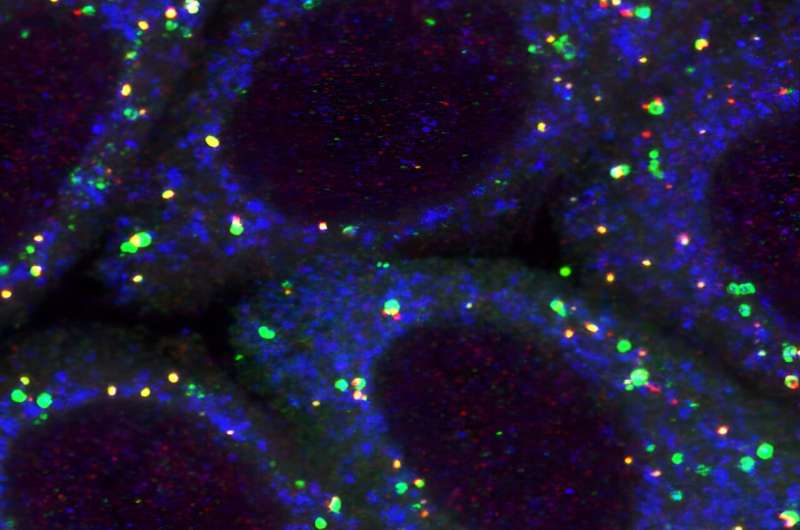
Mitochondria (blue) being targeted by mitophagy (green and red). Credit: WEHI
Parkinson’s disease is the world’s fastest growing neurological condition. Currently there are no drugs or therapies that slow or stop the progression of the disease.
In Australia, someone is diagnosed with Parkinson’s approximately every 30 minutes. Current estimates show there are more than 219,000 people living with Parkinson’s in Australia, a number forecast to double in the next 15 years.
WEHI’s Parkinson’s Disease Research Center has some of the world’s leading researchers tackling the problem using a multi-disciplinary collaborative approach.
New proteins linked to Parkinson’s pathway
Mitochondria are the energy generating machines in our cells and are kept healthy by mitophagy, which is the molecular process of removing or recycling damaged or dysfunctional mitochondria.
PINK1 and Parkin are two key genes involved in mitophagy, and mutations in these genes are linked to early-onset Parkinson’s disease.
Until the discovery of two proteins, NAP1 and SINTBAD, exactly how PINK1/Parkin mitophagy activation was regulated was unknown.
ooOOoo
We wish the scientists all the best as they delve into PD.
Personal musings on what ‘live for the day’ means.
Jeannie wakes early on in the morning; it’s one of the characteristics of Parkinson’s Disease (PD). So last Sunday morning I was washed and dressed by 5am (PST), and listening to the BBC’s World at One. (No connection with today’s post.)
Later on I started writing this post with a first look at what ‘live for the day’ means in the eyes of others. At first I wanted to research the phrase; imagine my surprise when I found out there wasn’t a consistent meaning.
Dictionary.com came up with Concentrate on the present, with little or no concern for the future.
Merriam-Webster gave live for meaning one of three things: lived for; living for; lives for.
The English-Collins dictionary, according to Wikipedia: The dictionary uses language research based on the Collins Corpus, which is continually updated and has over 4.5 billion words. But it did not easily give me any answer to my question.
Quora was too complicated for me to easily search for this phrase.
Thus I abandoned that approach.
I also did not reach out to friends and ask them what they thought of the saying. But, to me, that meaning from Dictionary.com seemed the closest to what I had in mind. So let me settle on that.
Concentrate on the present, with little or no concern for the future.
But how can Jeannie and me live without ‘concern for the future‘?
The list of things that we think about that involve the future is enormous. Many of the things are relatively minor, such as do we have enough food in the house, or petrol in the car, going on to do have I enough COB (Corn, Oats, Barley) to feed the deer that come here each morning, etc., etc.
Then there are future plans such as keeping next Tuesday clear (that is today, in fact) for Jeannie and Dordie to be out together for a few hours. Plus, in a few months time, my son is coming over to stay with us in April, and Richard coming in May. (Richard is a great British friend who was diagnosed with PD the same time as Jean.)
Then there is the task of keeping the trees within fifty feet of the house safe. That involves cutting down the trees that are getting old and trimming off the lower branches in the others. This is part of our desire to stay safe if a forest fire comes through this part of Merlin. We would be evacuated if that happened and part of our preparation is to have an ‘exit pack’ at the ready. Something else that affects our ‘concern for the future‘.
Finally in this list of introspections comes the ultimate end! I am in my 80th year and Jean and I find ourselves talking about death more often than we did at a younger age. Is that normal? I do not know. We are both humanists; I hope I will outlive Jean because I love her to pieces and want to be the last person she sees and embraces. It is one of the reasons that I go bike riding on a regular basis and staying as healthy as we can embraces the fact that we are both pescatarian and attend the local Club Northwest two days a week. Jeannie goes to the Rock Steady Class held at the Club.
So that is a pretty good set of reasons why living for the day is not viable.
ooOOoo
Footnote
We lost our Brandy yesterday morning. He went out for his usual ‘whatever’ at a little after 5am and after he had been back in the house for no more than a minute, he shook his head and went to the front door to be let out again! I thought he had gone out for a poo.
After I was washed and dressed, but it was still dark, I started to look for him aided by my big torch. I could not see him anywhere. To cut a long story short here we are at 4pm and he hasn’t surfaced. My speculation was that his head shake was a brain problem and then he lost all sense of where he was. To continue that speculation, I believe he ended up being swept away in Bummer Creek, that crosses our property just in from the main gate, and was drowned.
For most of us these days old age is part of the scene (and I am classifying old age as being over 70 years). Here are a few facts from the website of the World Health Organization.
Key facts
Worldwide obesity has nearly tripled since 1975.
In 2016, more than 1.9 billion adults, 18 years and older, were overweight. Of these over 650 million were obese.
39% of adults aged 18 years and over were overweight in 2016, and 13% were obese.
Most of the world’s population live in countries where overweight and obesity kills more people than underweight.
39 million children under the age of 5 were overweight or obese in 2020.
Over 340 million children and adolescents aged 5-19 were overweight or obese in 2016.
Obesity is preventable.
What are obesity and overweight Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health.
Body mass index (BMI) is a simple index of weight-for-height that is commonly used to classify overweight and obesity in adults. It is defined as a person’s weight in kilograms divided by the square of his height in meters (kg/m2).
Adults
For adults, WHO defines overweight and obesity as follows:
overweight is a BMI greater than or equal to 25; and
obesity is a BMI greater than or equal to 30.
BMI provides the most useful population-level measure of overweight and obesity as it is the same for both sexes and for all ages of adults. However, it should be considered a rough guide because it may not correspond to the same degree of fatness in different individuals.
World Health Organisation
This is the link for anyone who wants to use the BMI Calculator.
Now this is not a post about obesity or being overweight. It is a post taken from The Conversation about staying as healthy as one can in one’s older years.
ooOOoo
Steep physical decline with age is not inevitable – here’s how strength training can change the trajectory
Raise your hand if you regularly find yourself walking up a flight of stairs. What about carrying heavy bags of groceries? How about picking up your child or grandchild? Most of us would raise our hands to doing at least one of those weekly, or even daily.
As people age, it can become more and more difficult to perform some physical tasks, even those that are normal activities of daily living. However, prioritizing physical fitness and health as you get older can help you go through your normal day-to-day routine without feeling physically exhausted at the end of the day.
It can also help you continue to have special memories with your family and loved ones that you might not have been able to have if you weren’t physically active. For example, I ran two half-marathons with my dad when he was in his 60s!
I am an exercise physiologist who studies how people can use resistance training to improve human performance, whether it be in sports and other recreational settings, in everyday life, or both. I am also a certified strength and conditioning specialist. My career has given me the opportunity to design exercise programs for kids, college athletes and elderly adults.
Staying physically active as you get older doesn’t need to include running a half-marathon or trying to be a bodybuilder; it could be as simple as trying to get through the day without feeling winded after you go up a flight of stairs. Although our muscles naturally get weaker as we age, there are ways we can combat that to help improve quality of life as we get older.
From left are the author’s father, who was age 61 at the time, the author’s wife and the author after completing the Lincoln Half Marathon. Zachary Gillen, CC BY-NC-ND
Muscle loss and chronic disease
One of the most important parts of exercise programming, no matter who I am working with, is proper resistance training to build muscle strength. Some amount of age-related loss of muscle function is normal and inevitable. But by incorporating resistance training that is appropriate and safe at any ability level, you can slow down the rate of decline and even prevent some loss of muscle function.
In one of our team’s previous studies, we saw that otherwise healthy individuals with sarcopenia had issues delivering vital nutrients to muscle. This could lead to greater likelihood of various diseases, such as Type 2 diabetes, and slow down recovery from exercise.
Recent estimates suggest that sarcopenia affects 10% to 16% of the elderly population worldwide. But even if a person doesn’t have clinically diagnosed sarcopenia, they may still have some of the underlying symptoms that, if not dealt with, could lead to sarcopenia.
Strength training is key
So the question is, what can be done to reverse this decline?
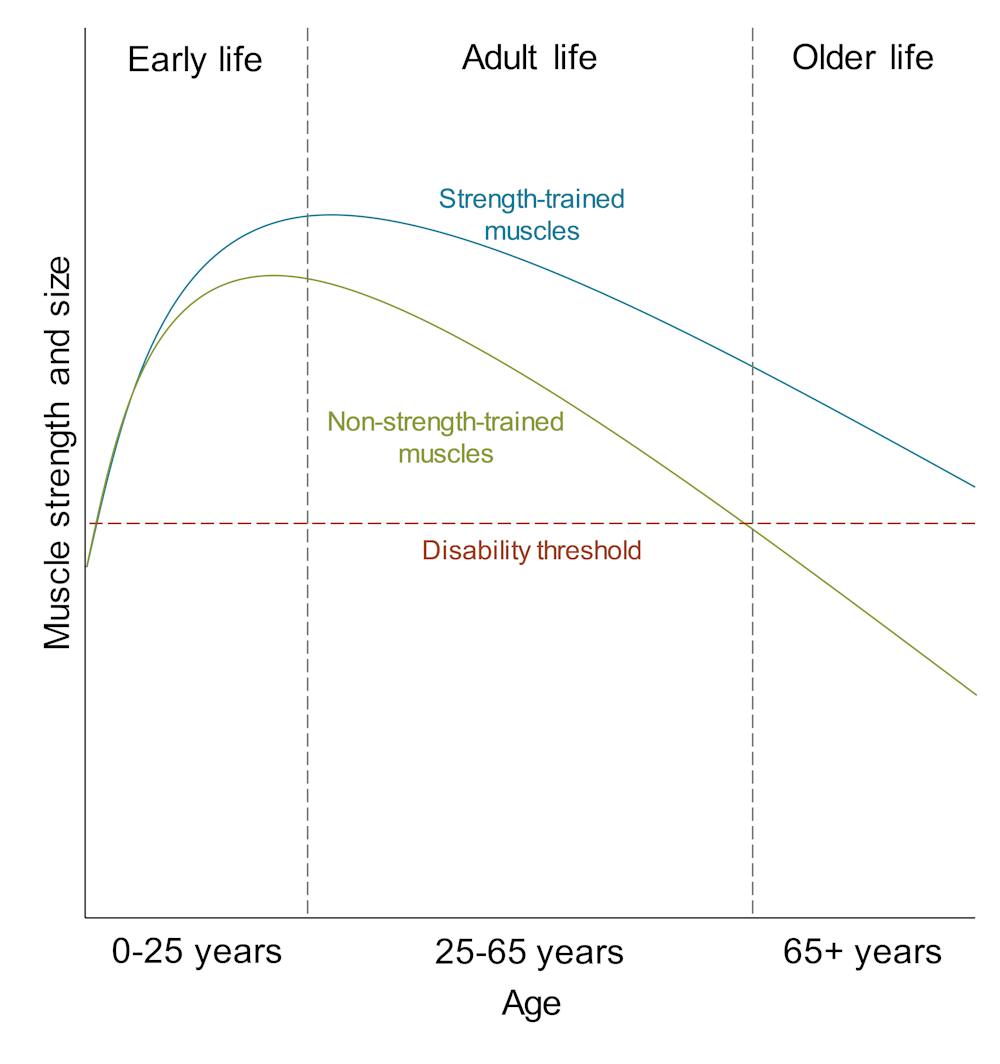
Recent evidence suggests that one of the key factors leading to sarcopenia is low muscle strength. In other words, combating or reversing sarcopenia, or both, may be best done with a proper resistance-training program that prioritizes improving strength. In fact, the decline in muscle strength seems to occur at a much faster rate than the decline in muscle size, underscoring the importance of proper strength training as people age.
Typical age-related changes in muscle strength and size with and without strength training. Zachary Gillen
Continuing to regularly strength train with moderate to heavy weights has been shown to be not only effective at combating the symptoms of sarcopenia but also very safe when done properly. The best way to make sure you are strength training properly is to seek out guidance from a qualified individual such as a personal trainer or strength and conditioning specialist.
Despite the clear benefits of strength training, it’s been shown that only about 13% of Americans age 50 and older do some form of strength training at least twice a week.
Finding what works for you
So how does a person properly strength train as they age?
The National Strength and Conditioning Association, a leading organization in advancing strength and conditioning around the world, states that for older adults, two to three days per week of strength training can be incredibly helpful for maintaining healthy muscle and bone and combating a number of chronic conditions.
The organization recommends that these workouts involve one to two exercises involving multiple joints per major muscle group, with six to 12 repetitions per set. These are done at an intensity of 50% to 85% of what’s known as one-repetition maximum – the most weight you could handle for a single repetition – with the exception of body weight exercises that use one’s own body weight as the resistance, such as pushups.
I would also recommend resting for about two to three minutes between sets, or even up to five minutes if the set was challenging. For older adults, particularly those age 60 and older, the National Strength and Conditioning Association guidelines suggest that a program like this be performed two to three days per week, with 24 to 48 hours between sessions.
An example of a strength training routine for older adults based on the National Strength and Conditioning Association guidelines
There are a great variety of exercises that could be done interchangeably in a strength training program like this.
The guidelines above are only one example out of many options, but they provide a framework that you can use to build your own program. However, I would highly recommend seeking out a professional in the field to give specific exercise programming advice that can be tailored to your own needs and goals as you age.
Following such a program would give your muscles an excellent stimulus to enhance strength, while also allowing enough recovery, a very important consideration as people age. You might think it looks like a huge time commitment, but an exercise routine like this can be done in less than an hour. This means that in less than three hours of strength training per week you can help improve your muscle health and reduce the risk of getting sarcopenia and associated health issues.
It’s also important to note that there is no one right way to do resistance training, and it needn’t involve traditional weight equipment. Group classes like Pilates and yoga or those that involve circuit training and work with resistance bands can all produce similar results. The key is to get out and exercise regularly, whatever that entails.
My wife, Jean, was diagnosed with Parkinson’s Disease (PD) in December, 2015. Many of you know that.
Fortunately at our local Club Northwest there was a group of PD sufferers who twice a week held a ‘Rock Steady Class’ under the instruction of a professional coach; Jean joined the group. It was a brilliant move for Jean and she gets a huge amount of care from being with them.
Luckily for me having to drive Jean into Club Northwest it made sense for me to sign up to a fitness class at the same time so I am put through a regular fitness routine under the coaching of Bruce. Plus I try and go bike riding three times a week.
In other words, we both try and stay as fit as we can.
Three promising developments in Parkinson’s research.
As I am sure most of you know Jean was diagnosed in having Parkinson’s Disease (PD) in late 2015 and from that moment on I have taken more than a superficial interest in PD. Especially as my best friend in England, Richard M. was similarly diagnosed in late 2015 – “the fickle finger of fate“.
So a recent Neuro Talk from the Parkinson’s Foundation is my contribution for today.
ooOOoo
Three Promising Developments in Parkinson’s Research
Every year, the Parkinson’s Foundation funds the most exciting and promising research ideas in the Parkinson’s disease (PD) field.
In our latest Neuro Talk, Chief Scientific Officer James Beck, PhD, is joined by three researchers whose studies were funded by the Parkinson’s Foundation. Their projects, which range from investigating environmental factors to understanding cognition, explain how research is helping us further our understanding of Parkinson’s.
What is the Parkinson’s Foundation? The Parkinson’s Foundation makes life better for people with Parkinson’s disease (PD) by improving care and advancing research toward a cure. In everything we do, we build on the energy, experience and passion of our global Parkinson’s community. Learn more on our website: https://www.parkinson.org/
ooOOoo
For those that wish to understand PD in a scientific manner, here is a quote from the PD:
What is Parkinson’s disease? Parkinson’s disease (PD) is a neurodegenerative, progressive disorder that affects predominately dopamineproducing neurons in a specific area of the brain called substantia nigra
You all know that Jeannie has Parkinson’s Disease but it is not without its shocks.
Yesterday, at about 3.30 am there was a crash in the kitchen. Jeannie had tripped up and fallen down. She was laying very awkwardly all crumpled up. I came into the kitchen immediately, saw her on the floor, saw that she was in agony but couldn’t lift her up without hurting her more. So I called an ambulance.
I followed the ambulance in our car shortly thereafter. Jean was admitted to the emergency room.
After Jean had been given an x-ray and pain meds later on she was transferred to Room 350 in the main hospital. I was told that she needed surgery on her right hip, maybe a hip replacement, and she will be in overnight.
I had returned home before noon to let the dogs out and to have some breakfast! Then I went back to Jeannie.
I stayed with her until nearly 3pm. Jean was due to have surgery at 4:45 pm.
What the longer term implications are I do not know. I sincerely hope the surgery is successful and Jean returns home.
Another day with this terrible disease!
P.S. In the early evening it felt so lonely. I cuddled the three dogs many times but it still felt as though my world had been turned upside down. I am writing this before 6pm so do not even want to think of being on my own in bed. The dogs are acutely aware of Jean’s absence and are doing their best to comfort me. Wonderful Brandy, Oliver and Cleo!
It affects so many but it is also a cruel disease.
Parkinson’s Disease (PD) is unique to each individual as it is a disease of the brain. Yet there are aspects of the disease that affect most and especially the people who are close to the PD sufferer.
Following Alzheimer’s disease, Parkinson’s disease (PD) is the second-most common neurodegenerative disorder in the United States. Most people diagnosed with PD are age 60 years or older, however, an estimated 5 to 10 percent of people with PD are diagnosed before the age of 50. Approximately 500,000 Americans are diagnosed with PD, but given that many individuals go undiagnosed or are misdiagnosed the actual number is likely much higher. Some experts estimate that as many as 1 million Americans have PD. Of course, given the progressive nature of the disabilities associated with PD, the disease affects thousands more wives, husbands, children, and other caregivers.
NINDS website
Jean was diagnosed in December, 2015 at the same time as my best friend in England, Richard Maugham.
More than 10 million people worldwide are living with PD!
Here is a video put out by Parkinson’s UK that is introduced as follows:
In this honest and often funny live talk Colin describes his experience with Parkinson’s and his hopes for the future.
So a wish on behalf of those countless other people: May there be a cure soon!
I was chatting to my very old friend, as in the number of years, Richard Maugham yesterday and shortly after the call he sent me an email with a link to a recent item on the BBC News website.
Most of you regulars know that Jeannie was diagnosed with Parkinson’s disease (PD) in December, 2015 and coincidentally at the same time Richard was also diagnosed with PD.
I’m sure there are a few who read this blog that either have PD of know or someone who has it.
ooOOoo
Prostate drug may slow Parkinson’s disease
By Michelle Roberts,
Health editor, BBC News online
17th September, 2019
A drug used to treat enlarged prostates may be a powerful medicine against Parkinson’s disease, according to an international team of scientists.
Terazosin helps ease benign prostatic hyperplasia (BPH) by relaxing the muscles of the bladder and prostate.
But researchers believe it has another beneficial action, on brain cells damaged by Parkinson’s.
They say the drug might slow Parkinson’s progression – something that is not possible currently.
Cell death
They studied thousands of patients with both BPH and Parkinson’s.
Their findings, published in the Journal of Clinical Investigation, suggest the alpha-blocker drug protects brain cells from destruction.
Parkinson’s is a progressive condition affecting the brain, for which there is currently no cure.
Existing Parkinson’s treatments can help with some of the symptoms but can’t slow or reverse the loss of neurons that occurs with the disease.
Terazosin may help by activating an enzyme called PGK1 to prevent this brain cell death, the researchers, from the University of Iowa, in the US and the Beijing Institute for Brain Disorders, China, say.
Clinical trials
When they tested the drug in rodents it appeared to slow or stop the loss of nerve cells.
To begin assessing if the drug might have the same effect in people, they searched the medical records of millions of US patients to identify men with BPH and Parkinson’s.
They studied 2,880 Parkinson’s patients taking terazosin or similar drugs that target PGK1 and a comparison group of 15,409 Parkinson’s patients taking a different treatment for BPH that had no action on PGK1.
Patients on the drugs targeting PGK1 appeared to fare better in terms of Parkinson’s disease symptoms and progression, which the researchers say warrants more study in clinical trials, which they plan to begin this year.
‘Exciting area’
Lead researcher Dr Michael Welsh says while it is premature to talk about a cure, the findings have the potential to change the lives of people with Parkinson’s.
“Today, we have zero treatments that change the progressive course of this neurodegenerative disease,” she says.
“That’s a terrible state, because as our population ages Parkinson’s disease is going to become increasingly common.
“So, this is really an exciting area of research.”
‘Disease modifying’
Given that terazosin has a proven track record for treating BPH, he says, getting it approved and “repurposed” as a Parkinson’s drug should be achievable if the clinical trials go well.
The trials, which will take a few years, will compare the drug with a placebo to make sure it is safe and effective in Parkinson’s.
Co-researcher Dr Nandakumar Narayanan, who treats patients with Parkinson’s disease said: “We need these randomised controlled trials to prove that these drugs really are disease modifying.
“If they are, that would be a great thing.”
Prof David Dexter from Parkinson’s UK said: “These exciting results show that terazosin may have hidden potential for slowing the progression of Parkinson’s, something that is desperately needed to help people live well for longer.
“While it is early days, both animal models and studies looking at people who already take the drug show promising signs that need to be investigated further.”
Interestingly, if one goes to the website of the JCI then one reads the following on the ‘About’ page:
The Journal of Clinical Investigation is a premier venue for discoveries in basic and clinical biomedical science that will advance the practice of medicine.
“Happiness resides not in possessions, and not in gold, happiness dwells in the soul.”
So wrote the philosopher Democritus who was born in 460 BCE (although some claim his year of birth was 490 BCE). He acquired fame with his knowledge of the natural phenomena that existed in those times and history writes that he preferred a contemplative life to an active life, spending much of his life in solitude. The fact that he lived to beyond 100 suggests his philosophy didn’t do him any harm.
OK! Before I continue, please let me state, as before, that I write to you purely as Jean’s husband. I have no medical skills or knowledge at all and if you are at all affected by any of the following make an appointment to see your own doctor!
The crux of this post is Jean’s relationship with a naturopathic doctor at a practice in Seattle. The practice is Seattle Integrative Medicine (SIM) and a number of the doctors at SIM specialise in patients with PD. That’s how Jean was connected with Dr. Laurie Mischley. (Dr. M)
When one goes to the web page for Dr. M one reads:
Dr M conducted tests including testing her ear wax*, extensive blood analysis and an analysis of a sample of Jean’s hair.
* Dr. M has a dog that can reliably smell the presence of PD in human ear wax!
The favourite drug for those with PD is Levadopa. Within 48 hours of Jean taking Levadopa she had a serious allergic response to that drug.
Back to Dr. M’s tests. All three tests were non-indicative of PD. A while later, in a subsequent telephone conversation, Dr. M wondered if Jean really did have PD. She recommended a referral to the Oregon Health and Science University (OHSU) in Portland. Specifically to their Department of Neurology and to Dr. John Nutt. His background may be viewed here. From which one notes:
John Nutt, M.D.
Co-founder and Director Emeritus of the OHSU Parkinson Center and Movement Disorders Program
Professor of NeurologySchool of Medicine Expertise
Neurology
Special focus on Parkinson’s and Movement Disorders
Jean’s appointment was at 08:30 on Tuesday, 9th July. In terms of the timeline of all of us, Jean was diagnosed as suspected of having PD in December, 2015.
Dr. Nutt saw us promptly at 8:30 and immediately revealed a listening, caring attitude. He also quietly admitted that he had been a doctor specialising in neurology and movement disorders for 39 years! There was no question in my mind that we had landed in front of the ideal physician under these circumstances.
Over the next hour, Dr. Nutt examined Jean in a great number of ways. From her stretching her arms out, Dr. Nutt examining Jean’s arm joints, watching Jean walk along the corridor outside his examining room, and much more.
Eventually he paused and looked us both in the eyes. He then spoke quietly: “Jean is displaying a number of classic symptoms of Parkinson’s disease. I have no doubt that Jean does have the disease.”
Of course it wasn’t long before I mentioned Laurie Mischley’s opinion that Jean might not have PD. But Dr. Nutt was very clear with his reply. Namely that PD cannot be determined from hair and blood tests alone and that the potential sufferer must be examined physically.
Dr. Nutt asked me if I had noticed that when Jean held her arms straight out in front of her at shoulder height the tremors in her right hand ceased yet when she was relaxed with her hands in her lap the tremor in her right hand was very noticeable? I had not spotted that.
“Paul, that is a classic Parkinson’s characteristic.”
Dr. Nutt went on to say that watching Jean walk gave him another indicator of PD. Because although Jean walks well she doesn’t swing her arms. Classic PD!
Without doubt, Dr. Nutt’s impression was Idiopathic Parkinson’s disease.
But Dr. Nutt also said that Jean was doing incredibly well taking into account that she would have been suffering from the disease for at least 4 to 5 years and that her commitment to lots of exercise including her RockSteady class, that he was aware of, and her vegetarian diet was critically valuable.
It was now time to turn to medication for Jean. Dr. Nutt said that of all the drugs Levadopa was the ideal to combat the loss of dopamine in the brain. He was puzzled as to why Jean had had such a strong allergic reaction to the drug. He wondered if it was a reaction to the Carbidopa that in the USA was so often a component of the Levadopa medication. If so, that could be worked around. Dr. Nutt even mused that he had known of a patient who was allergic to the yellow dye that is sometimes in that medication.
His medication plan for Jean was for her to start on a 1/2 tablet of carbidopa-levadopa 25-100 mg tablets just once a day and if she has no bad reaction in a week then up that to two 1/2 tablets a day. If no adverse effects then increase by 1/2 tablet every week until taking 1 tablet three time a day.
So here we are, a week and a day after we returned from OHSU and, touch wood, Jean has had no adverse effects and is now on two 1/2 tablets a day.
But a postscript to that consultation with Dr. Nutt. At the very end I said that I had two questions. Dr. Nutt welcomed me to ask them.
“My first question is to do with the trend for PD. Is it getting worse?”
“Paul, here in the USA we are seeing a slow but definite decline in the incidence of Parkinson’s. What was your second question?”
“Dr. Nutt, my next question was whether or not science was pointing a finger at the cause of Parkinson’s disease?”
He replied without hesitating: “We are seeing a strong correlation between pesticides and Parkinson’s disease.”
Upon hearing that, Jeannie immediately spoke up recalling her times out in the Mexican fields when the crop-spraying aircraft flew right overhead. Adding that she had at times been drenched by the spray.
But, please, let us not forget: Association is not causation!
That’s enough for today. Because I was going on to include information about the importance of exercise. About managing one’s life really well. About the importance of diet and overall health. In a sense, not just for PD sufferers but for anyone the wrong side of 60 years old!!
That will be coming along soon!
I will close by thanking everyone at OHSU. The quality of care, attentiveness and experience of the staff backed by world-class resources was second-to-none!
To be in their system, so to speak, is a privilege.
I deliberately chose that sub-heading because Wednesday’s post is going into the details of a consultation that Jean had with Dr. John Nutt, MD, a neurologist at the Oregon Health and Science University (OHSU) in Portland, last Monday, 9th July.
Jean wants me to share the details with you because it is quite likely, nay, almost certainly, that some of you dear readers know of someone close to you that has Parkinson’s Disease (P.D.).
The balance of today’s post, to be continued tomorrow, is a reposting of something I published on February 24th, 2016.
ooOOoo
Life is a one-way track.
Those of you who follow this place on a regular basis know that last Friday I published a post under the title of Friday Fondness. You will also know that later that same day I left this comment to that post:
Sue, and everyone else, we returned from seeing Dr. Lee, the neurologist, a little under two hours ago. Dr. Lee’s prognosis is that Jean is showing the very early signs of Parkinson’s disease, and Jean is comfortable with me mentioning this.
Everyone’s love and affection has meant more than you can imagine. I will write more about this next week once we have given the situation a few ‘coatings of thought’.
Jean sends her love to you all!
Thus, as heralded, I am going to write some more.
You would not be surprised to hear that the last few days have been an emotional roller-coaster, for both Jean and me. Including on Monday Jean hearing from our local doctor here in Grants Pass, OR, that a recent urine test has shown that Jean has levels of lead in her bones some three times greater than the recommended maximum. While our doctor is remaining open-minded it remains to be seen whether Jean is exhibiting symptoms of lead poisoning, whether the lead is a possible cause of the Parkinson’s disease (PD), see this paper, or whether it is a separate issue to be dealt with.
However, I want to offer some more from the consultation that Jean had with the neurologist Dr. Eric Lee last Friday. Shared with the full support of Jean who has read the whole of today’s post yesterday evening; as she does with every post published in this place.
But before so doing, please understand that while I was present throughout the complete examination of Jean, what you are about to read carries no more weight than that of any casual onlooker. If you are at all affected by any of the following make an appointment to see your own doctor!
Jean’s examination lasted for about an hour. It consisted of a great number of checks and tests on how her body responded to many different tests and stimulations. At the end of the examination Dr. Lee said that while he wasn’t 100% certain the balance of probability was that Jean was demonstrating the very early signs of PD. For example, showing such signs as walking and not swinging both arms in a normal, balanced manner. Or having a very slow blink rate. Then she was exhibiting some difficulty with rapid finger-to-thumb taps.
However, Dr. Lee did say that Jean was at the very early stages of PD and that we would have to wait another six months to see if the PD indicators were firming up. He also said that he had PD patients who had had the disease for twenty, even thirty years. Some of the general indicators that PD is progressing include a stooped gait, decreasing size of handwriting, and a quieter speaking tone. The NINDS website has more information on this. Here’s a little of what they explain about PD:
What is Parkinson’s Disease?
Parkinson’s disease (PD) belongs to a group of conditions called motor system disorders, which are the result of the loss of dopamine-producing brain cells. The four primary symptoms of PD are tremor, or trembling in hands, arms, legs, jaw, and face; rigidity, or stiffness of the limbs and trunk; bradykinesia, or slowness of movement; and postural instability, or impaired balance and coordination. As these symptoms become more pronounced, patients may have difficulty walking, talking, or completing other simple tasks. PD usually affects people over the age of 60. Early symptoms of PD are subtle and occur gradually. In some people the disease progresses more quickly than in others. As the disease progresses, the shaking, or tremor, which affects the majority of people with PD may begin to interfere with daily activities. Other symptoms may include depression and other emotional changes; difficulty in swallowing, chewing, and speaking; urinary problems or constipation; skin problems; and sleep disruptions. There are currently no blood or laboratory tests that have been proven to help in diagnosing sporadic PD. Therefore the diagnosis is based on medical history and a neurological examination. The disease can be difficult to diagnose accurately. Doctors may sometimes request brain scans or laboratory tests in order to rule out other diseases.
But here’s the good news regarding my darling wife – there are three things that Dr. Lee strongly recommends:
Hang on to a positive mental attitude for the body actively produces dopamine when in a positive mental state.
At least 30-minutes of good aerobic exercise three times a week,
And physiotherapy.
In addition, Dr. Lee said to always THINK BIG! Big in voice, big in attitude, big in stature.
Finally, let me share with you what was posted on the Visible Procrastinations blog back in 2009. Reposted with the author’s permission.
ooOOoo
That article first seen on Visible Procrastinations will be republished tomorrow. Once more I must stress that I write to you purely as Jean’s husband. I have no medical skills or knowledge at all and if you are at all affected by any of the following make an appointment to see your own doctor!





Sue, and everyone else, we returned from seeing Dr. Lee, the neurologist, a little under two hours ago. Dr. Lee’s prognosis is that Jean is showing the very early signs of Parkinson’s disease, and Jean is comfortable with me mentioning this.
Everyone’s love and affection has meant more than you can imagine. I will write more about this next week once we have given the situation a few ‘coatings of thought’.
Jean sends her love to you all!